Fillable Form VA 10 - 10EZ
The VA 10-10EZ Form is used by veterans to apply for enrollment in the VA health care system. The information provided is used to determine a veteran's eligibility for medical benefits.
What is Form VA 10-10EZ?
Form VA 10-10EZ, Application for Health Benefits, is used by veterans to apply for enrollment in the Veteran Affairs (VA) health care system. The information that will be provided by a veteran in this form will be used to determine his or her eligibility to claim certain medical benefits. After completing this form, the department will send the veteran a letter to his or her home address outlining his or her priority group, enrollment, and other important health-related concerns.
How to fill out Form VA 10-10EZ?
Taxpayers can download and print a PDF copy of the VA Form 20 572 Form from the United States Department of Veteran Affairs (US DVA) website that they can manually complete. They can also fill out VA Form 20 572 Form electronically on PDFQuick.
To fill out the VA 20-572 Form, you must provide the following information:
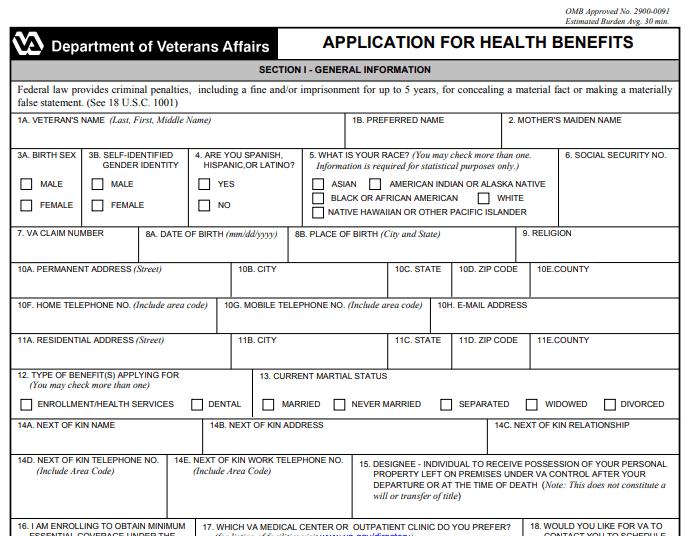
Section I. General Information
Box 1a. Veteran’s Name
Enter your full legal name using the format: Last Name, First Name, Middle Name.
Box 1b. Preferred Name
Enter the name you prefer to use.
Box 2. Mother’s Maiden Name
Enter the full legal maiden name of your mother.
Box 3a. Birth Sex
Mark the appropriate box which corresponds to your birth sex. You may select:
Box 3b. Self-Identified Gender Identity
Mark the appropriate box which corresponds to your self-identified gender identity. You may select:
Box 4
Mark YES if you are Spanish, Hispanic, or Latino; otherwise, mark NO.
Box 5. Race
Mark the appropriate box which corresponds to your race. You may select more than one box:
This information will be required for the purpose of statistics only.
Box 6. Social Security Number (SSN)
Enter your social security number (SSN).
Box 7. Veteran Affairs (VA) Claim Number
Enter your claim number from the Veteran Affairs (VA).
Box 8a. Date of Birth
Enter the date of your birth using the format: Month, Day, Year.
Box 8b. Place of Birth
Enter the place of your birth including the city and the state.
Box 9. Religion
Enter your religion.
Box 10a. Permanent Address
Enter your permanent address including the street.
Box 10b. City
Enter your city.
Box 10c. State
Enter your state.
Box 10d. ZIP Code
Enter your ZIP code.
Box 10e. County
Enter your county.
Box 10f. Home Telephone Number
Enter your home telephone number.
Box 10g. Mobile Telephone Number
Enter your mobile telephone number.
Box 10h. Email Address
Enter your email address.
Box 11a. Residential Address
Enter your residential or home address.
Box 11b. City
Enter your city.
Box 11c. State
Enter your state.
Box 11d. ZIP Code
Enter your ZIP code.
Box 11e. County
Enter your county.
Box 12. Type of Benefits
Mark the appropriate box which corresponds to the type of benefits you are applying for. You may mark more than one box.
Box 13. Current Marital Status
Mark the appropriate box which corresponds to your current marital status. You may select:
Box 14a. Next of Kin Name
Enter the full legal name of your next of kin.
Box 14b. Next of Kin Address
Enter the presidential or home address of your next of kin.
Box 14c. Next of Kin Relationship
Enter the relationship you have with your next of kin.
Box 14d. Next of Kin Telephone Number
Enter the telephone number of your next of kin.
Box 14e. Next of Kin Work Telephone Number
Enter the work telephone number of your next of kin.
Box 15. Designee
Enter the full legal name of the individual who has been assigned to receive possession of your personal property that has been left on the premises under VA control.
Box 16
Mark YES if you are enrolling to obtain minimum essential coverage under the affordable care act; otherwise, mark NO.
Box 17
Enter the name of the Veteran Affairs (VA) medical center or outpatient clinic you prefer.
Box 18
Mark YES if you would like the VA to contact you to schedule your first appointment; otherwise, mark NO.
Section II. Military Service Information
Box 1a. Last Branch of Service
Enter your last branch of service in the military.
Box 1b. Last Entry Date
Enter your last entry date in the military.
Box 1c. Future Discharge
Enter your future discharge in the military.
Box 1d. Last Discharge Date
Enter your last discharge in the military.
Box 1e. Discharge Type
Enter the type of your discharge.
Box 1f. Military Service Number
Enter your military service number.
Box 2. Military History
Answer the questions by marking YES or NO.
Question a
Mark YES if you are a purple heart award recipient; otherwise, mark NO.
Question b
Mark YES if you are a former prisoner of war; otherwise, mark NO.
Question c
Mark YES if you served in a combat theater of operations after November 11, 1998; otherwise, mark NO.
Question d
Mark YES if you were discharged or retired from the military for a disability incurred in the line of duty; otherwise, mark NO.
Question e
Mark YES if you are receiving disability retirement pay instead of VA compensation; otherwise, mark NO.
Question f
Mark YES if you served in Asia during the Gulf War between August 2, 1990 and November 11, 1998; otherwise, mark NO.
Question g
Mark YES if you have a VA service connected rating; otherwise, mark NO. If you marked YES, enter your rated percentage.
Question h
Mark YES if you served in Vietnam between January 9, 1962 and May 7, 1975; otherwise, mark NO.
Question i
Mark YES if you were exposed to radiation while serving in the military; otherwise, mark NO.
Question j
Mark YES if you received nose and throat radium treatments while serving in the military; otherwise, mark NO.
Question k
Mark YES if you served on active duty at least 30 days at Camp Lejune from August 1, 1953 through December 31, 1987; otherwise, mark NO.
Applicant for Health Benefits
Veteran’s name
Enter your full legal name.
Social security number (SSN)
Enter your social security number (SSN).
Section III. Insurance Information
Box 1
Health insurance company name
Enter the name of your health insurance company.
Address
Enter the address of your health insurance company.
Telephone number
Enter the telephone number of your health insurance company.
Box 2. Name of policy holder
Enter the full legal name of your policy holder.
Box 3. Policy number
Enter your policy number.
Box 4. Group code
Enter your group code.
Box 5
Mark YES if you are eligible for Medicaid; otherwise, mark NO.
Box 6a
Mark YES if you are enrolled in Medicare Hospital Insurance Part A; otherwise, mark NO.
Box 6b
Enter the effective date for your enrollment using the format: Month, Day, Year.
Section IV. Dependent Information
Box 1. Spouse’s name
Enter the full legal name of your spouse.
Box 1a. Spouse’s social security number (SSN)
Enter the social security number (SSN) of your spouse.
Box 1b. Spouse’s date of birth
Enter the date of birth of your spouse.
Box 1c. Spouse’s self-identified gender identity
Mark the appropriate box which corresponds to the self-identified gender identity of your spouse. You may select:
Box 1d. Date of marriage
Enter the date of your marriage.
Box 1e. Spouse’s address and telephone number
Enter the residential or home address and telephone number of your spouse.
Box 2. Child’s name
Enter the full legal name of your child.
Box 2a. Child’s date of birth
Enter the date of birth of your child.
Box 2b. Child’s social security number (SSN)
Enter the social security number (SSN) of your child.
Box 2c. Date child became your dependent
Enter the date when your child has been your dependent.
Box 2d. Child’s relationship to you
Mark the appropriate box which corresponds to the relationship you have with your child. You may select:
Box 2e
Mark YES if the child was permanently and totally disabled before the age of 18; otherwise, mark NO.
Box 2f
Mark YES if the child is between 18 and 23 years of age and has attended school last year; otherwise, mark NO.
Box 2g
Enter the amount of expenses your dependent child has paid for college, vocational rehabilitation, and training.
Box 3
Mark YES If your spouse or dependent child did not live with you last year and you have provided support; otherwise, mark NO.
Section V. Employment Information
Box 1a. Veteran’s employment status
Mark the appropriate box which corresponds to your employment status. You may select:
Box 1b. Date of retirement
Enter your date of retirement.
Box 1c. Company name
Enter the name of your company.
Box 1d. Company address
Enter the address of your company.
Box 1e. Company phone number
Enter the phone number of your company.
Section VI. Previous Calendar Year Gross Annual Income of Veteran, Spouse, and Dependent Children
Item 1
Enter your gross annual income from employment and enter the amount your spouse and child have received.
Item 2
Enter your net income from your farm, ranch, and properties or businesses and enter the amount your spouse and child have received.
Item 3
Enter any other incomes you may have and enter the amount your spouse and child have received.
Section VII. Previous Calendar
Item 1
Enter the total amount of your unreimbursed medical expenses that has been paid by you or your spouse.
Item 2
Enter the total amount you paid last calendar year for funeral and burial expenses.
Item 3
Enter the total amount you paid last calendar year for your college or vocational educational expenses.
Section VII. Consent to Copays and to Receive Communications
Signature of applicant
Affix your signature.
Date
Enter the current date of signing.