Fillable Form FSDL-705
Wyoming Drivers License Application Form is used by an individual that needs to apply for a drivers license one year upon moving to the state or renewing an expired drivers license.
What is Form FSDL-705?
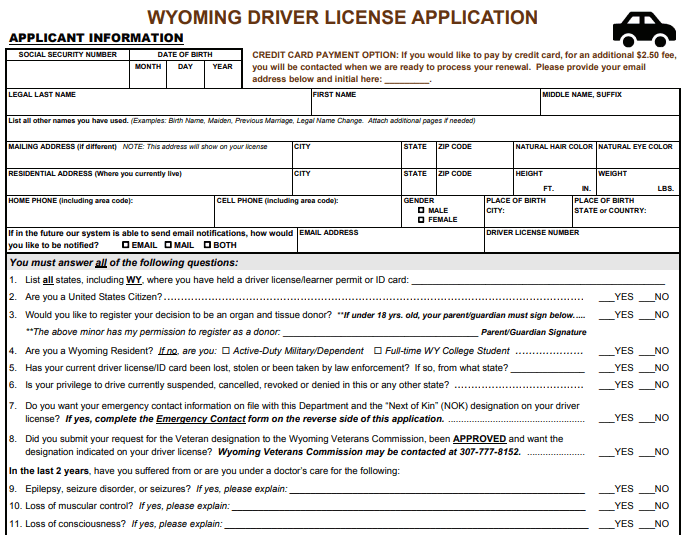
Form FSDL-705, Wyoming Driver License Application, is a state-level form in the state of Wyoming. Form FSDL-705 is issued by the Wyoming Department of Transportation and used by eligible residents of the state of Wyoming to apply for a driver’s license. New drivers and new residents who wish to drive within the state of Wyoming need to have a valid Wyoming driver’s license.
Form FSDL-705 asks for identifying information, including the applicant’s full legal name, Social Security Number (SSN), addresses, and contact information.
Where to get Form FSDL-705?
The Wyoming Department of Transportation provides a blank copy of Form FSDL-705. You may also visit the official Wyoming Department of Transportation website to download and print a copy that you can fill out manually. Alternatively and for your convenience, you may electronically fill out Form FSDL-705 on PDFQuick.
How to fill out Form FSDL-705?
To fill out Form FSDL-705, you will need to supply your personal information and answer driving-related questions.
Form FSDL-705 is a two-page document. You must answer all the questions that apply to you. The first page is where you will provide the Wyoming Department of Transportation with your personal information and answer driving-related and health-related questions.
Answer all the fields accurately and truthfully to avoid any problems and delays with your application to change your address. You must not deliberately provide any false information as doing so is unlawful and may result in penalties and imprisonment.
Social Security Number
Enter your Social Security Number (SSN).
Date of Birth
Enter your date of birth in the following format: Month, Day, Year.
Legal Last Name
Enter your legal last name.
First Name
Enter your first name.
Middle Name, Suffix
Enter your middle name and suffix.
List all other names you have used
Enter all the names you have legally used. You may attach additional pages if needed.
Mailing Address
Enter your mailing address, including City, State, ZIP Code. Your mailing will show on your license.
Residential Address
Enter your residential address where you currently live, including City, State, ZIP Code.
Natural Hair Color
Enter your natural hair color.
Natural Eye Color
Enter your natural eye color.
Height
Enter your height in feet and inches.
Weight
Enter your weight in pounds.
Home Phone
Enter your home phone number, including the area code.
Cell Phone
Enter your cell phone number, including the area code.
Gender
Mark the appropriate box to determine your gender. You may select:
Place of Birth City
Enter the name of the city where you were born.
Place of Birth State or County
Enter the name of the state or county where you were born.
If in the future our system is able to send email notifications, how would you like to be notified?
Mark the appropriate box to determine how you would like to be notified when the Wyoming Department of Transportation is already able to send email notifications. You may select:
Email Address
Enter your active email address.
Driver License Number
Enter your driver’s license number.
Item 1
Enter all states, including Wyoming, where you have held a driver’s license or learner permit, or identification card.
Item 2
Mark YES if you are a United States Citizen; otherwise, mark NO.
Item 3
Mark YES if you would like to register your decision to be an organ and tissue donor; otherwise, mark NO. If you are under 18 years old, your parent or guardian must affix his or her signature to give his or her permission to register you as a donor.
Item 4
Mark YES if you are a Wyoming resident; otherwise mark NO. If you marked NO, mark the appropriate box to determine your type of residency. You may select:
Item 5
Mark YES if your current driver’s license or identification card has been stolen or been taken by aw enforcement; otherwise, mark NO. If YES, enter the state.
Item 6
Mark YES of your privilege to drive currently suspended, canceled, revoked, or denied in this or any other state; otherwise, mark NO.
Item 7
Mark YES if you want your emergency contact information on file with this Department and the “Next of Kin” (NOK) designation on your driver’s license; otherwise, mark NO. If you answered YES, complete the Emergency Contact form on the second page of Form FSDL-705.
Item 8
Mark YES if you submitted your request for the Veteran designation to the Wyoming Veterans Commission and have been approved, and you want the designation on your driver’s license; otherwise, mark NO.
Item 9
Mark YES if in the last 2 years you have suffered from or are you under a doctor’s care for epilepsy, seizure disorder, or seizures; otherwise, mark NO. If you answered YES, explain.
Item 10
Mark YES if in the last 2 years you have suffered from or are you under a doctor’s care for the loss of muscular control; otherwise, mark NO. If you answered YES, explain.
Item 11
Mark YES if in the last 2 years you have suffered from or are you under a doctor’s care for the loss of consciousness; otherwise, mark NO. If you answered YES, explain.
Item 12
Mark YES if in the last 2 years you have suffered from or are you under a doctor’s care for the loss or impairment of a limb; otherwise, mark NO. If you answered YES, explain.
Applicant Signature
Affix your signature.
Date
Enter the date you signed the form.
Parent/Guardian Signature
If a minor applicant, affix the signature of the parent or guardian.
Date
If a minor applicant, enter the date the parent or guardian signed.
Print the Name of the Person Signing for Minor
Enter the name of the parent or guardian if the applicant is a minor.
Mark the appropriate box to determine the parent or guardian’s relationship with the minor applicant. You may select:
Emergency Contact Information
Relationship to Applicant
Enter the emergency contact’s relationship to the applicant.
Emergency Contact Full Name
Enter the emergency contact’s full name.
Contact Phone
Enter the emergency contact’s phone number, including the area code.
Emergency Contact Residential Address
Enter the emergency contact’s residential address.
Alternate Phone
Enter the emergency contact’s alternate phone number, including the area code.
Applicant Name
Enter the name of the applicant.
Date
Enter the date the form was completed.